Accessory Nerve Definition
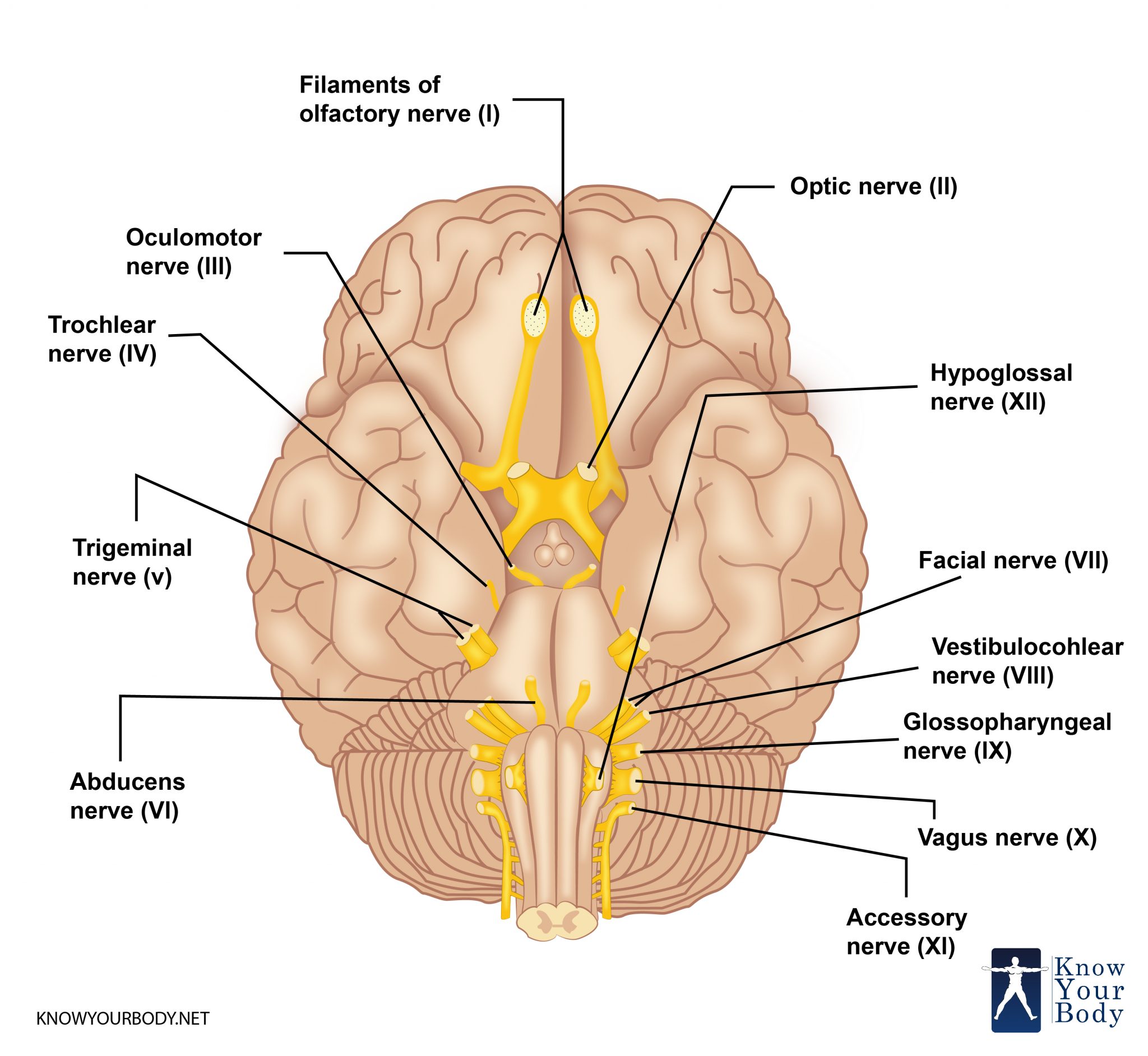
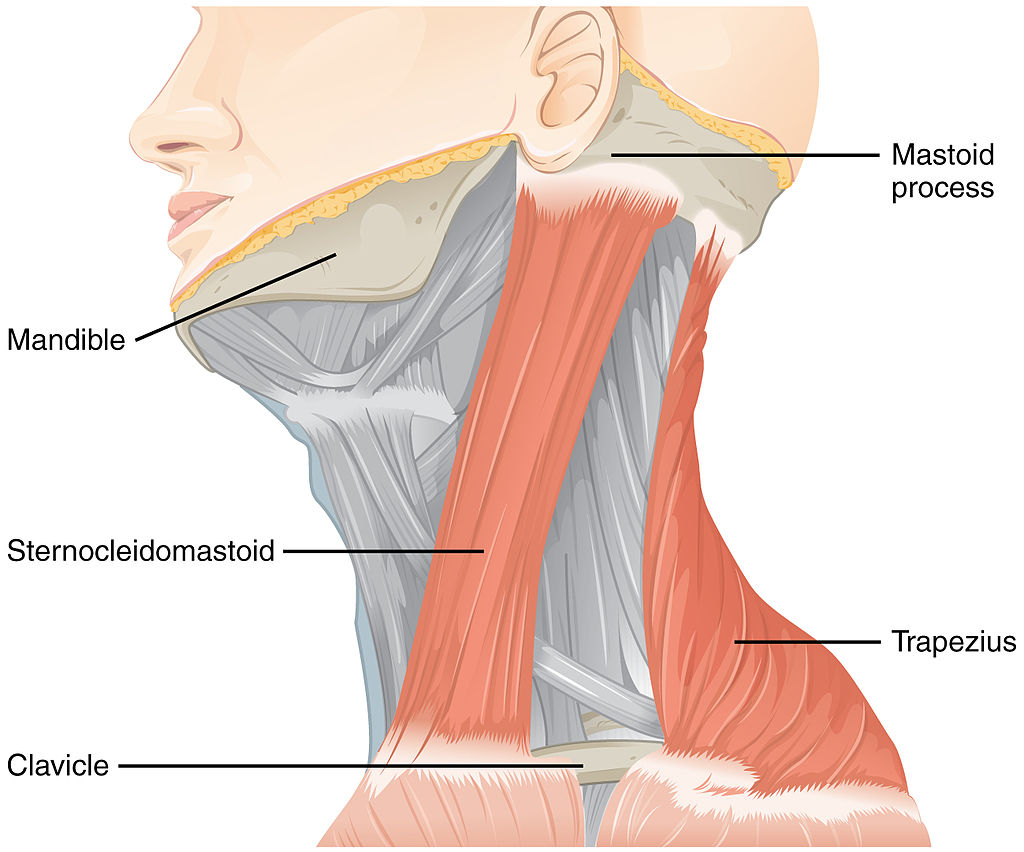
Amongst the twelve pairs of the cranial nerve in the brain, the eleventh pair of cranial nerve (CN11) is called the Accessory Nerve. It supplies innervation to the sternocleidomastoid muscles that helps in tilting and rotating of the head and trapezius muscles that helps in performing various actions such as shoulder elevation and abduction motion (motions that move a structure away from the center of the body) of the arm.
Accessory Nerve Location and Origin
The accessory nerve offers motion functions to the sternocleidomastoid muscles that extend from the neck and move to trapezius and then extends to the upper back and shoulder. It is a cranial nerve that serves the trapezius and sternocleidomastoid muscles. It is deemed as the 11th muscle of twelve pairs of the cranial nerves, or just cranial nerve XI. Being a part of this it is believed to originate in the brain.
Accessory Nerve Location
Accessory Nerve Structure
The spinal accessory nerve’s fibers originate from the neurons located in the upper spinal cord. It is the part where the spinal cord starts at the junction to medulla oblongata to the level of C6. The fibers link to create roots, rootlets, and the spinal accessory nerve.
It enters into the skull from the foramen magnum, which is a big opening at the skull base. The nerve moves near the inner wall of the skull near the jugular foramen. After this the nerve routes through jugular foramen with vagus nerves and glossopharyngeal.
The structure of accessory nerve is divided into three parts:
Nucleus
The spinal accessory nerve is formed by fibers of lower motor neurons situated in the upper areas of the spinal cord. The group of neurons is known as the nucleus. It is situated in the lateral aspect of the anterior area of the spinal cord and extends from where the spinal cord starts through the level of C6. The end part of high cervical segments seems to be regular with nucleus ambiguous from medulla oblongata, which is the area dividing the cranial part of the accessory nerve.
Variation
The necessary nerve intersects the interior jugular vein across the level of posterior belly of the digastric muscle. The vein is in front of around 80% people and is at the back of 20% people.
Conventionally, it was considered that accessory nerve has a small cranial aspect that diminishes from the medulla and then connects with spinal accessory aspect before separating off to the nerve to link the vagus nerve. But there was a study introduced in 2007 that stated that in most of the people, the cranial component does not mark any different link to the spinal aspect. The roots of such different aspects were separated by a fibrous sheath.
Development
The basal plate in the embryonic spinal components C1-C6 derives the accessory nerve.
Accessory Nerve Anatomy
The anatomy of the accessory nerve can be studied by detailing its parts. The Accessory Nerve is divided into two parts:
The first one is called the Spinal Accessory Nerve that originates in the neurons located in the upper spinal cord (medulla oblongata). The fibers of the Spinal Accessory Nerve join together to form rootlets, roots, and the spinal Accessory Nerve itself. It then enters the skull in the human body through the foramen magnum which is like a large opening in the base of the skull. From the skull, it goes through the jugular foramen with the glossopharyngeal and vagus nerves. The Spinal Accessory Nerve is a unique one that is it is known to be the only cranial nerve that enters and exits the skull.
The cranial portion or the cranial Accessory Nerve is smaller than the Spinal Accessory Nerve. It arises from the medulla oblongata’s lateral parts. From the jugular foramen, it then leaves the cranium and connects to the spinal portion of the main Accessory Nerve. Once it leaves the skull, the cranial portion combines with CN X or the vagus nerve at the inferior ganglion.
Accessory Nerve Functions
Let us look at the motor functions of the Accessory Nerve. The Accessory Nerve helps with motor control of the sternocleidomastoid and trapezius muscles.
The trapezius muscle is the one that controls the actions like shrugging the shoulders. The action comes from the opposite side of the brain. The upper part of the trapezius muscle elevates the scapula when it contracts.
The nerve fiber sternocleidomastoid controls the action of turning the head. It is considered that this is capable of changing sides twice which means it is controlled by the brain on the same side of the body. Its contraction leads to turning of the head on the opposite side. This can be explained by understanding that the head turns to that side of the brain from where it receives visual information.
Accessory Nerve Blood Supply
Accessory nerve supplies blood to the trapezius muscles and the sternocleidomastoid muscles. It is the 11th of twelve pairs of the cranial nerve.
Accessory Nerve Action
It is well-noted fact that surgeries and medical procedures are the root cause of injuries to the spinal Accessory Nerve. Two common surgeries known as the neck dissection and cervical lymph node biopsy are responsible for a spinal Accessory Nerve damage.
The treatment options are varied in number when an iatrogenic (surgery done by the surgeon) spinal Accessory Nerve is injured. An intraoperative procedure or a postoperative procedure can help in the recuperation of a damaged spinal Accessory Nerve. One such example is the Eden-Lange procedure wherein the most of the remaining purposeful shoulder muscles are surgically relocated, mostly used in the treatment of trapezius muscle palsy.
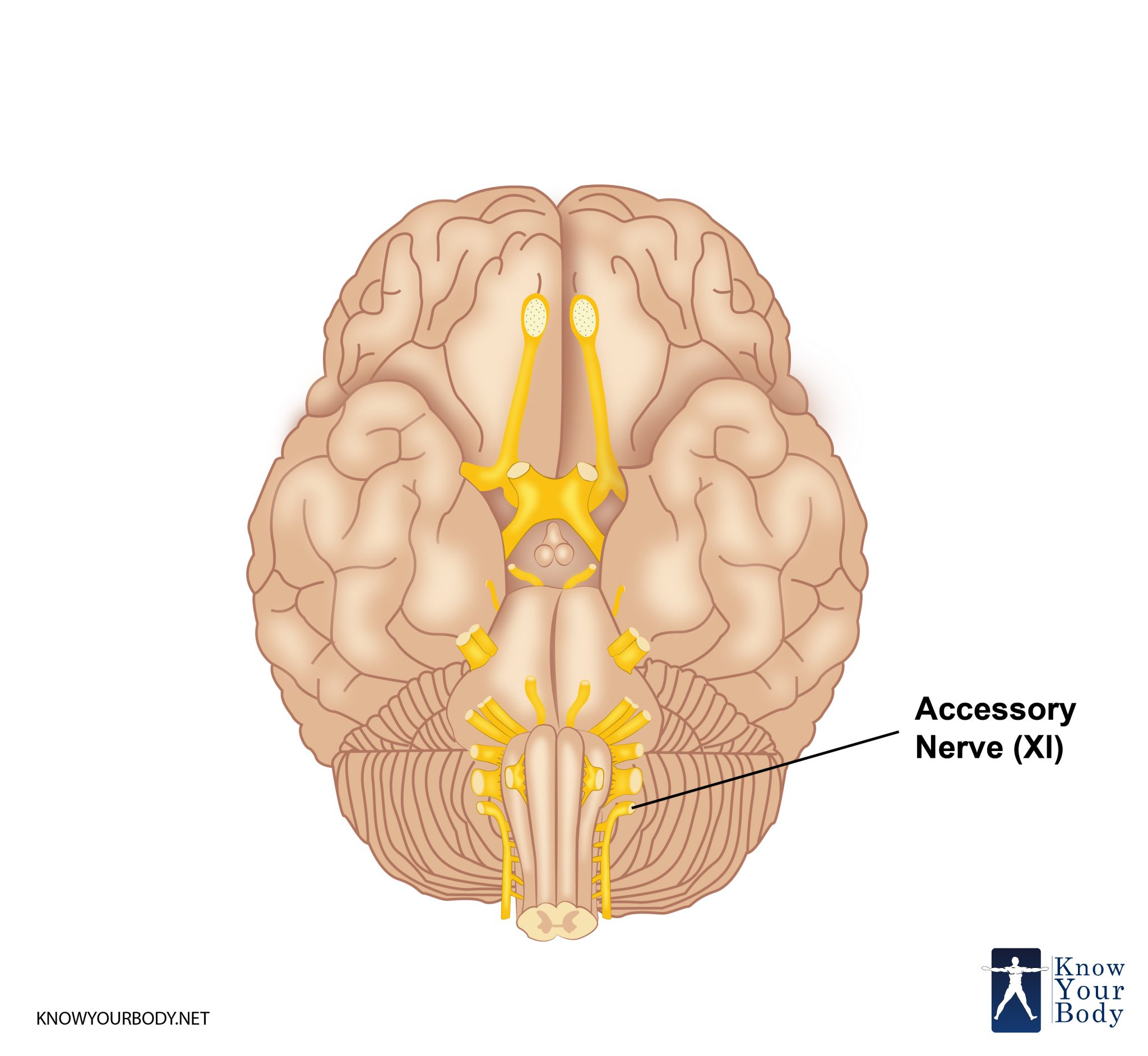
Accessory Nerve Pictures
Accessory Nerve Clinical Complications
The clinical complication of accessory nerve involves testing the nerve by analyzing the function of sternocleidomastoid muscles and trapezius.
An examination is conducted to test the trapezius muscle. The patient is asked to shrug the shoulders with some resistance. Another examination is performed to test sternocleidomastoid muscle that involves the patient to rotate their head to turn right or left against resistance.
If trapezius is weak then this would result in one-sided injury to the accessory nerve. When a person experiences weakness in turning the head then it suggest injury of the contralateral accessory nerve. The weak leftward turn indicates weak sternocleidomastoid muscle, while the right side weakness indicates weak left sternocleidomastoid muscle and hence the left area of spinal accessory.
The major reasons for clinical complications of the accessory nerve are trauma, tumors, surgery, and compressing of the jugular foramen.
Accessory Nerve Diseases
The major disease experienced in the accessory nerve is its injury. This usually occurs because of following reasons:
- Neck surgery like lymph node surgery or neck dissection
- Resulted from penetrating or blunt trauma, which in some cases is highly spontaneous.
- Damaging of the route of the nerve that disturbs the overall functioning of the nerve
- Intentionally removal of nerve in radical neck dissections that is performed mainly during a surgical procedure, particularly when a person experiences cancer
- Weakness of trapezius muscle or pain in the neck.
When there is injury or damage to the accessory nerve then this can lead to atrophy, depression of shoulder girdle, and abnormal movement of the shoulder, weakened abduction, and protruding scapula. Such situations can lead to other medical issues like torticollis.
Diagnosis
The patient is asked to rotate their head, shrug their shoulders and upon observation of any signs of discomfort or pain in performing the above-mentioned actions, it is understood that there is a course of treatment and therapy has to be provided. A common cause of Accessory Nerve damage is due to a surgery performed or a medical procedure performed during operations such as node biopsy of the cervical lymph which causes damage to the nerve. Mostly termed as palsy of the Accessory Nerve, this can result in muscle wasting and paralysis of the sternocleidomastoid. An asymmetrical neckline also occurs due to damage to the muscle.
Treatment
The treatment of accessory nerve can be conducted in three different types:
- Conservative Management Approach
- Physical Therapy
- Surgical Repair
Conservative Management or Rehabilitation Therapy
This therapy involves treatment of spinal accessory nerve through occupational and physical therapy. It is great to relieve the pain. The aim of this treatment is to promote gradual movement of the nerve and to ensure proper functioning of related body parts.
During the treatment, a patient is suggested to avoid carrying hefty weights on the affected region. The patient is also requested to hook thumbs in the pants pocket on the affected areas that can enhance the relief. Sometimes the patient is also suggested to use an arm sling to combat pain.
Physical Therapy
This is another crucial way to treat the injured accessory nerve. This treatment aims to regain or maintain the passive ROM from shoulder. It limits the stiffness of shoulder capsule and ligaments that can occur with improper alignment of the shoulder.
Surgical Treatment
This treatment is suggested only when it is obvious and confirmed injury of the accessory nerve. The doctor suggests surgical treatment when a patient experiences dense paralysis, distressing subjective symptoms, severe pain, the absence of clinical improvement after multiple examinations, and the nerve does not show any contraction.
Some prominent surgical measures adopted are neurolysis, cable graft, primary nerve anastomosis, and Eden-Lange muscle transfer.
Frequently Asked Questions
What purpose does Accessory Nerve offer?
One of the most significant cranial nerves, Accessory Nerve helps in controlling the movement of various neck muscles. It also provides the motor function to the sternocleidomastoid muscle, which broadens the neck and trapezius, also the upper back and shoulder. Any damage to the Accessory Nerve can cause a considerable amount of dysfunction to shoulder’s performance.
What is Accessory Nerve Palsy?
It is a complication that may occur post a surgery performed on the neck’s posterior triangle shaped area that is located between the sternocleidomastoid and trapezius on both sides of the neck.
What is the clinical examination procedure for damage in Accessory Nerve?
Any damage to the Accessory Nerve can cause muscle wasting in a patient. The doctor asks a patient to rotate their head and shrug their shoulders. A long-standing damage will be observed simply by signs of muscle wasting in the sternocleidomastoid and trapezius mostly in cases of long-standing nerve damage.
No comments yet.